Foot Pain: 8 Things That Actually Help — for Runners, Desk Workers, and Kids
- Freya Moran

- Jun 1
- 6 min read
The alarm goes off. You put your feet on the floor and your first conscious thought of the day is: that pain. Or you're on kilometre four of your run and your shin starts talking to

you. Or your ankle rolls on a slightly uneven kerb — for the third time this year. Foot problems are democratically distributed: they show up in marathon runners, in people who sit at desks for eight hours in rigid shoes, in children who are just learning what their bodies can do, and in everyone in between.
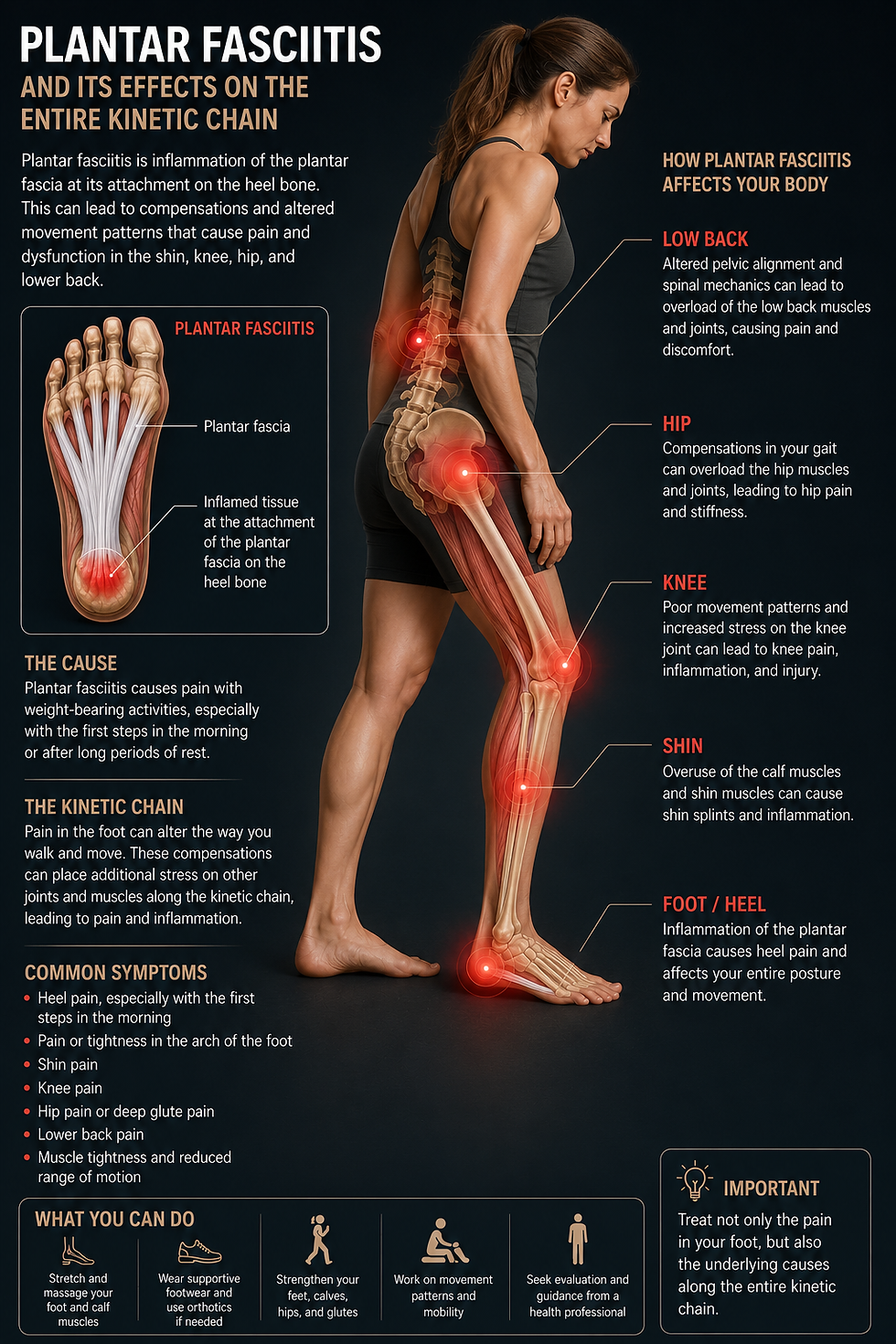
What unites them is that the foot is the foundation of every movement. And when the foundation is compromised, the structure above it adapts — usually in ways that eventually cause knee pain, hip pain, or back pain. This post gives you eight things that genuinely work, explains what doesn't help as much as people hope, and clarifies when it makes sense to stop self-managing and get a proper assessment.
For detailed information on our approach, see the Foot Pain Munich page.
Why foot pain rarely self-resolves without intervention
The foot depends on a precise interaction between mobile joints, strong intrinsic muscles, and well-conditioned connective tissue. When one part of this system is compromised — a restricted ankle joint, weak arch-stabilising muscles, a tight calf — the load distributes unevenly. The overloaded structure becomes painful. The body compensates. The compensation pattern becomes habitual. And the original problem, even if the acute pain subsides, remains structurally unchanged — waiting for the next trigger.
8 things that actually help
1. Eccentric calf loading — the most underused exercise for foot pain
The gastrocnemius-Achilles-plantar fascia system is a functional unit. The calf muscle drives tension through the Achilles tendon and into the plantar fascia with every step. A tight, shortened calf complex is the primary mechanical driver of most plantar fasciitis, Achilles tendinopathy, and many shin splint presentations. Stretching helps — but eccentric loading is more effective.
The exercise: stand with your toes on a step, heel hanging free. Using both feet to go up, lower on the affected leg only. Slow, controlled descent. 3 sets of 15 repetitions, twice daily. It should feel like work, not pain. This is the Alfredson protocol, one of the most evidence-supported exercises in musculoskeletal rehabilitation — and it works for plantar fasciitis and Achilles tendinopathy alike.

2. Foot sole massage — before the first step
For plantar fasciitis sufferers, the worst moment of the day is that first contact with the floor. The plantar fascia has shortened overnight and is suddenly loaded. Two minutes of foot sole massage with a tennis ball before you get up — rolling from heel to toe, slowly, with light-to-moderate pressure — mobilises the fascia, improves local circulation, and significantly reduces start-up pain. Do this before standing, not after. Daily, not occasionally.
3. The short foot exercise — activating what shoes have switched off
The intrinsic foot muscles — the small muscles inside the foot that dynamically stabilise the arch — are progressively underactivated in anyone who spends significant time in supportive footwear. They're doing less and less work while the shoe does it for them. The short foot exercise specifically reactivates them.
Sit with the foot flat. Without curling your toes, try to shorten the foot from front to back — drawing the ball of the foot toward the heel, lifting the arch slightly off the ground. Hold 5 seconds. 10 repetitions. It will feel difficult at first; that's diagnostic. As it becomes easier, progress to standing, then single-leg standing. This exercise is appropriate for a child building foot strength for the first time, a desk worker rehabilitating plantar fasciitis, and a runner preventing overpronation — the progression is the same, the starting point differs.
4. Ankle dorsiflexion mobilisation — the missing piece
Restricted dorsiflexion — the ability to bring the foot upward — is one of the most consistently found impairments in patients with plantar fasciitis, shin splints, and knee pain. When the ankle can't flex properly, the foot compensates with increased pronation and elevated fascial tension. Self-test: place the foot 10 cm from a wall. Keeping the heel flat, push the knee forward to touch the wall. If the heel lifts before the knee reaches the wall, dorsiflexion is restricted.
Self-mobilisation: kneel with the foot flat, then drive the knee forward over the foot and back repeatedly for 2 minutes. If restriction persists, manual joint mobilisation by a chiropractor often achieves in one session what weeks of stretching cannot.
5. Go barefoot — on appropriate surfaces
Walking or standing barefoot on natural, uneven surfaces is the most effective intrinsic muscle training available. Grass, sand, gravel, wooden floors — every surface variation activates the small foot muscles that shoes suppress. Begin with 10 to 15 minutes daily if you're not accustomed to it. For children: barefoot at home and on natural outdoor surfaces whenever possible. Children who regularly walk and play barefoot on varied surfaces develop stronger foot muscles and better movement patterns than those whose feet are constantly supported. The school shoes can stay — the rest of the time, the feet benefit from working on their own.
6. Use orthotics correctly — as a bridge, not a destination
Orthotics serve a legitimate purpose: they redistribute load during acute presentations, reduce pain, and allow tissues to heal. What they don't do is strengthen muscles or restore joint mobility. A patient using orthotics without a concurrent exercise programme is becoming progressively more dependent on external support while the underlying deficit continues. Our approach: orthotics as a temporary tool during the acute phase, always combined with a progressive loading programme aimed at making the orthotic redundant. This applies to adults and children equally. If you've been wearing the same orthotics for three-plus years with no change in programme, that's worth revisiting.
7. Manage running load — the 10 percent rule
The single most common cause of shin splints, plantar fasciitis, and stress injuries in runners is training load that increases faster than the tissue can adapt. The 10 percent rule: don't increase weekly distance by more than 10 percent from one week to the next. This applies after injury returns, after holidays, and after any break of more than two weeks. When pain appears during a training build, reducing volume by 30 to 50 percent (not stopping entirely) and switching to softer surfaces is the appropriate response. Complete rest often produces more deconditioning than benefit; the goal is to find the load the tissue tolerates while it adapts.
8. Address hip weakness — the upstream cause of many foot problems
Weak hip abductors and external rotators are consistently found in runners and active patients with plantar fasciitis, shin splints, and overpronation. A weak hip allows the knee to collapse inward during loading, which increases pronation at the foot and elevates fascial tension. A simple test: stand on one leg and observe the knee. Does it drift inward? That's the hip, not the foot. Exercises: clamshells, side-lying hip abduction, and single-leg Romanian deadlifts address the upstream deficit. You may find your foot pain improves significantly when your hip strength does.
What doesn't help as much as people hope
Cortisone injections as first-line treatment: Valuable for acute inflammatory flares. Don't address restricted joints, weak muscles, or poor mechanics. Repeated injections can weaken tendon tissue. A bridge, not a solution.
Rest alone: Foot tissue heals under load, not without it. The right load — progressive, calibrated, appropriate to the tissue's current capacity — is therapeutic. Total rest often means returning to activity with weaker, less load-tolerant tissue than before.
Shock wave therapy without rehabilitation: Shock wave can break the pain cycle in chronic tendinopathy. Without concurrent strength and coordination work, the causative factors remain. Pain returns.
When to stop self-managing and see a chiropractor
Two to three weeks of consistent self-management without a clear improvement trend is the threshold. Foot pain that keeps recurring, or that is spreading in its impact (affecting gait, causing knee or hip pain), warrants a proper structural assessment.
At our Munich practice, we combine gait analysis, joint assessment, soft tissue work, and a progressive loading programme into a coherent treatment plan — one that addresses not just where the pain is, but why the structure was overloaded in the first place. No referral needed, and short-notice appointments are available. Information on what a first appointment involves and our fees is on the pricing page.
Warning signs: when foot pain needs urgent attention
Go to A&E or call emergency services if:
You cannot bear weight after a fall or twist
There is visible deformity of the ankle or foot
You have diabetes and an open wound on your foot
You experience sudden, unexplained numbness in the foot
The bottom line
Feet are extraordinarily capable — but only when the joints move freely, the muscles are strong, and the movement patterns are sound. The eight strategies above address all three dimensions in a way that passive supports and rest cannot. For lasting resolution, the structure needs to be treated, not just offloaded.
If you're in Munich and ready to address what's actually driving your foot pain, see the full Foot Pain Munich page, or book a first appointment directly — no referral required, often available at short notice.
Related pages:


